- Messages
- 4,442
- Reaction score
- 1,973
- Points
- 113
By Glenn Koslowski
Typically starting at about the age of 30, a man’s testosterone levels drop by about 10% every decade. Together with that, sex binding hormone globulin (SHBG) levels start to increase, “trapping” much of the circulating testosterone and making it effectively unavailable to exert its expected effects on the body. The resulting difference between the total testosterone and the bound, unavailable is what we call free or “bioavailable” testosterone and, more importantly than the total levels of the hormone, plays a major role in the health, drive, quality of life and performance of an individual.
Every man will experience a decline in free testosterone as age comes, but some men will experience it harder and faster than others. The reason for that may be physical, psychological, environmental or as a result of years of natural-production suppression due to steroid usage when younger. When this happens, these men will go through a variety of negative symptoms that can severely impact their day-to-day life and even expose their health to the long-term risks of low testosterone. Some of these risks are:
Other options include the use of transdermal gels and creams, patches, pellets and implants. To stay within physiological testosterone levels range, you will need to check the concentration and bioavailability of the chosen method in order to work out your dose.
However, it may not be that simple. Some individuals may need to use other medications during their TRT programs. These include:
Overall, the health benefits to be gained overwhelmingly seem to support Testosterone replacement when you consider the beneficial effects to energy levels, metabolism, muscle mass/functionality, and even blood chemistry and cardiac health, if done correctly.
Typically starting at about the age of 30, a man’s testosterone levels drop by about 10% every decade. Together with that, sex binding hormone globulin (SHBG) levels start to increase, “trapping” much of the circulating testosterone and making it effectively unavailable to exert its expected effects on the body. The resulting difference between the total testosterone and the bound, unavailable is what we call free or “bioavailable” testosterone and, more importantly than the total levels of the hormone, plays a major role in the health, drive, quality of life and performance of an individual.
Every man will experience a decline in free testosterone as age comes, but some men will experience it harder and faster than others. The reason for that may be physical, psychological, environmental or as a result of years of natural-production suppression due to steroid usage when younger. When this happens, these men will go through a variety of negative symptoms that can severely impact their day-to-day life and even expose their health to the long-term risks of low testosterone. Some of these risks are:
- Cardiovascular disease
- Cancer
- Diabetes
- Osteoporosis
- Depression
- Alzheimer’s
- Erectile Dysfunction
- Metabolic Syndrome
- Abdominal fat: waist circumference above 40 inches in men; 35 inches in women.
- Elevated blood pressure: greater than 140/90 mmHg.
- Decreased HDL “good” cholesterol: less than 45 mg/dL in men; less than 50 mg/dL in women.
- Elevated triglycerides: greater than 150 mg/dL.
- Elevated fasting glucose: greater than 110 mg/dL.
- Frequent emotional changes
- Diminished sex drive
- Some form of erectile dysfunction (or less rigid erections)
- Decreased morning erections
- Decreased strength and/or muscle mass
- Decreased feeling of well-being
- Reduced mental quickness and sharpness
- Decreased energy, strength and endurance
- Less desire for activity and exercise
- Increased body fat
- Night sweats and trouble sleeping
- Some level of depression and irritability
- Loss of enthusiasm for daily life
Other options include the use of transdermal gels and creams, patches, pellets and implants. To stay within physiological testosterone levels range, you will need to check the concentration and bioavailability of the chosen method in order to work out your dose.
However, it may not be that simple. Some individuals may need to use other medications during their TRT programs. These include:
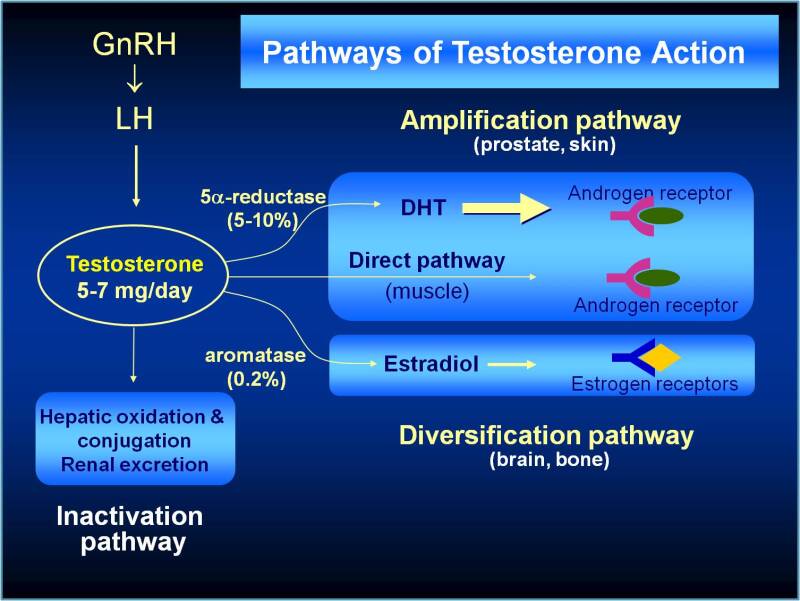
- Aromatase inhibitors (Anastrozole/Exemestane): AI’s block the conversion of testosterone into estrogen. TRT patients who suffer estrogen elevations above the top of normal range are often given an aromatase inhibitor.
- Selective Estrogen Receptor Modulators (SERMs), (Nolvadex/Tamoxifen): SERMs hinder the action but not the production of estrogen. In TRT contexts, this drug is usually taken to counter the physical manifestations of estrogen-related problems like gynecomastia.
- Human Chorionic Gonadotropin (hCG): even at TRT does, Testosterone supplementation suppresses natural production. Over time, this can lead to testicular atrophy. hCG helps restore and maintain Testosterone production and testicular size by mimicking LH and stimulating the production and release of natural Testosterone.
- 5-Alpha Reductase Inhibitors (Finasteride, Dutasteride/ Propecia, Proscar): These drugs are specific inhibitors of the 5a-reductase, the enzyme responsible for conversion of testosterone to dihydrotestosterone (DHT). In men, DHT has its own pros and cons. DHT is three times more potent than Testosterone, doesn’t aromatize to estrogen, and is associated with high libido. However, it’s also linked to male pattern baldness, acne, and prostate cancer.
Overall, the health benefits to be gained overwhelmingly seem to support Testosterone replacement when you consider the beneficial effects to energy levels, metabolism, muscle mass/functionality, and even blood chemistry and cardiac health, if done correctly.